
F HOW DO WE GRADE (ASSESS) DIABETIC RETINOPATHY?
1 The Photographic Gold Standard – The Airlie House Grading System
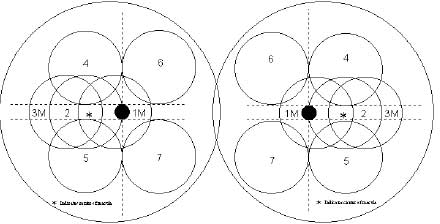
The development of the Airlie House grading system in 1969 enabled diabetic retinopathy to be assessed in a systematic method. With this grading system, seven-field stereoscopic photographs are taken of each fundus and the various lesions of diabetic retinopathy are graded according to standardised examples.
This system was used in two landmark trials that have defined modern day ophthalmic treatment of diabetic retinopathy- the Diabetic Retinopathy Study (DRS) and the Early Treatment of Diabetic Retinopathy Study (ETDRS). The DRS looked at whether scatter or pan-retinal laser photocoagulation altered the natural history of proliferative retinopathy. The ETDRS addressed the timing of scatter or pan-retinal laser photocoagulation to prevent or retard the progression of diabetic retinopathy and the effect of focal laser therapy on “clinically significant macular oedema”. These trials went on to modify the Airlie House system in the light of their findings.
FUNDUS PHOTOGRAPHIC RISK FACTORS FOR PROLIFERATIVE RETINOPATHY
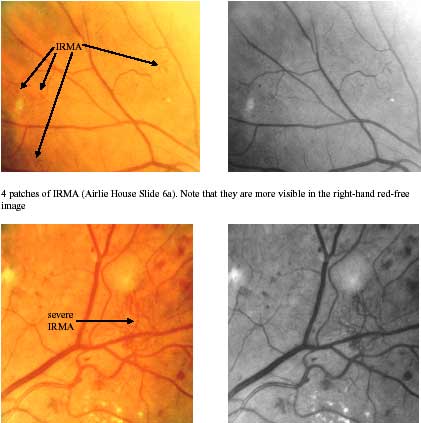
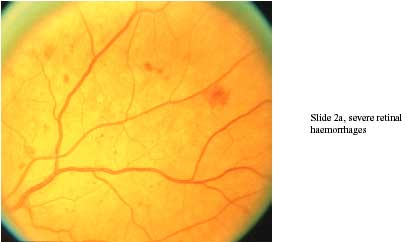
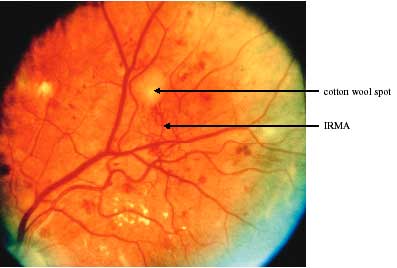
The ETDRS looked at fundus photographic risk factors for the development of proliferative retinopathy. The baseline severity of haemorrhages and/or microaneurysms, IRMAs, venous beading, cotton wool spots, hard exudates and the rate of progression to proliferative diabetic retinopathy (PDR) at one, three and five year follow up, were considered. One-year progression rates to PDR according to the baseline severity of the retinopathy are shown in the following figures (Early Treatment Diabetic Retinopathy Study Research Group 1991). The maximum severity of each feature was recorded using the following terminology: definitely present (D), moderate (M), severe (S) and very severe (VS). As well as the maximum severity of each feature, the number of Airlie House fields involved by each feature was also recorded.
Haemorrhages and/or Microaneurysms. One-year progression to proliferative diabetic retinopathy (PDR).
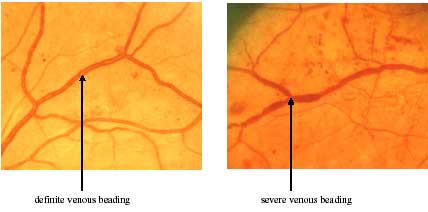
It can be seen that one-year progression rates increased fourfold or more with increasing severity of haemorrhages and/or microaneurysms, IRMAs and venous beading.
If venous beading was definitely present at baseline then 40.5% of eyes progressed to PDR by one year. Once IRMA and cotton wool spots were definitely present, 22% and 19.4% of eyes respectively progressed to PDR by one year.
However, there was little or no relationship between hard exudate formation and the development of proliferative retinopathy. Similarly, cotton wool spots on their “own” without the additional presence of IRMA, severe retinal haemorrhages or venous beading did not increase the risk of developing proliferative retinopathy. The presence of venous beading in any one photographic field was the most powerful predictor. Thus, it can be concluded that the most sensitive early predictors of the development of PDR are retinal haemorrhages/microaneurysms. Venous beading is more specific but fairly insensitive, while the specificity and sensitivity of IRMA falls in between the two.